Current Trends in the UK and the US
More or less as I was posting my previous piece, the UK government was publicly rolling back on the idea that the aim of ‘herd immunity’ was the optimal strategy in the face of the Coronavirus epidemic. At the same time it published the scenario modelling of the Imperial College COVID-19 Response Team, which contained the following passage.
In addition, even if all patients were able to be treated, we predict [under a mitigation strategy] there would still be in the order of 250,000 deaths in GB, and 1.1-1.2 million in the US. In the UK, this conclusion has only been reached in the last few days, with the refinement of estimates of likely ICU demand due to COVID-19 based on experience in Italy and the UK (previous planning estimates assumed half the demand now estimated) and with the NHS providing increasing certainty around the limits of hospital surge capacity.
Yet, as I described in my previous post, a figure in the region of 250,000 deaths could have been reached by somewhat simpler calculation.
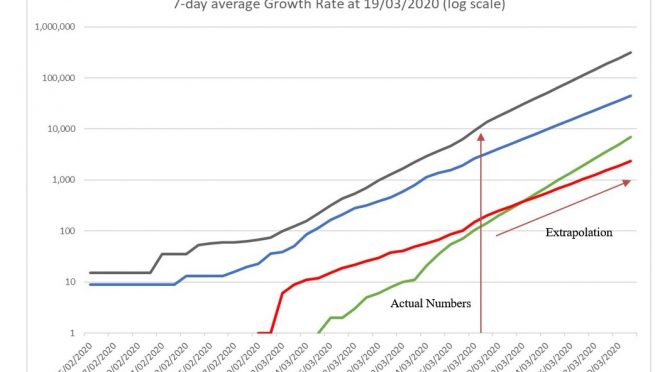
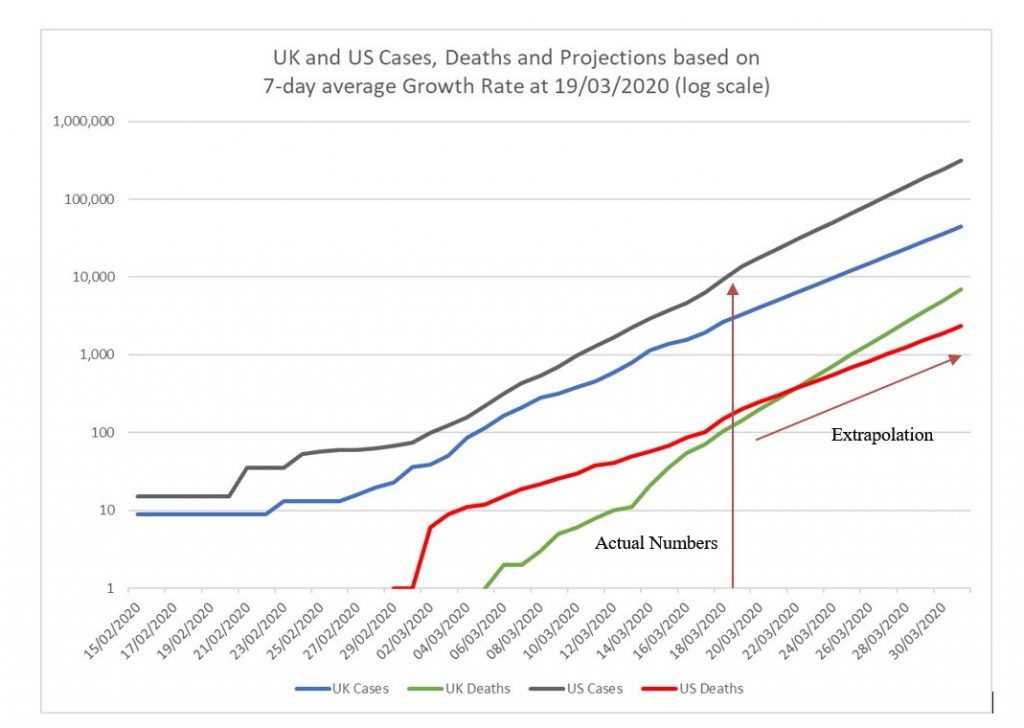
There is little sign of any alteration to the trajectory I outlined previously. The UK growth in cases over the last 7 days averages at around 0.25, whereas that in the US is close to 0.3. This means that new confirmed cases each day in the UK are around a quarter of the total cases from the day before, but in the US this is closer to one third. These differences may represent policy changes in each country, with the UK restricting testing to hospitalised cases, and the US attempting to ramp up testing from its previous relatively low level. We can project these rates of growth into the future however to suggest that the UK will have reached 10,000 cases in around five days, and the US 100,000 cases in about 1 week (Chart 1). Over the last few days the UK death rate has risen alarmingly, currently running at around 0.35 (35% additional deaths each day), considerably higher than the US mortality growth rate which as would be expected appears to be converging on the case growth rate. If this trend were to continue, the UK would have experienced 1,000 Covid-19 deaths in 5 days time, 1 day earlier than the US. It’s not clear why the UK death rate should be increasing so rapidly; maybe because of the lag in time between case detections and deaths, maybe because of the populations initially infected. The most concerning reason would be that even at this early stage the NHS is being stretched beyond capacity by the epidemic.
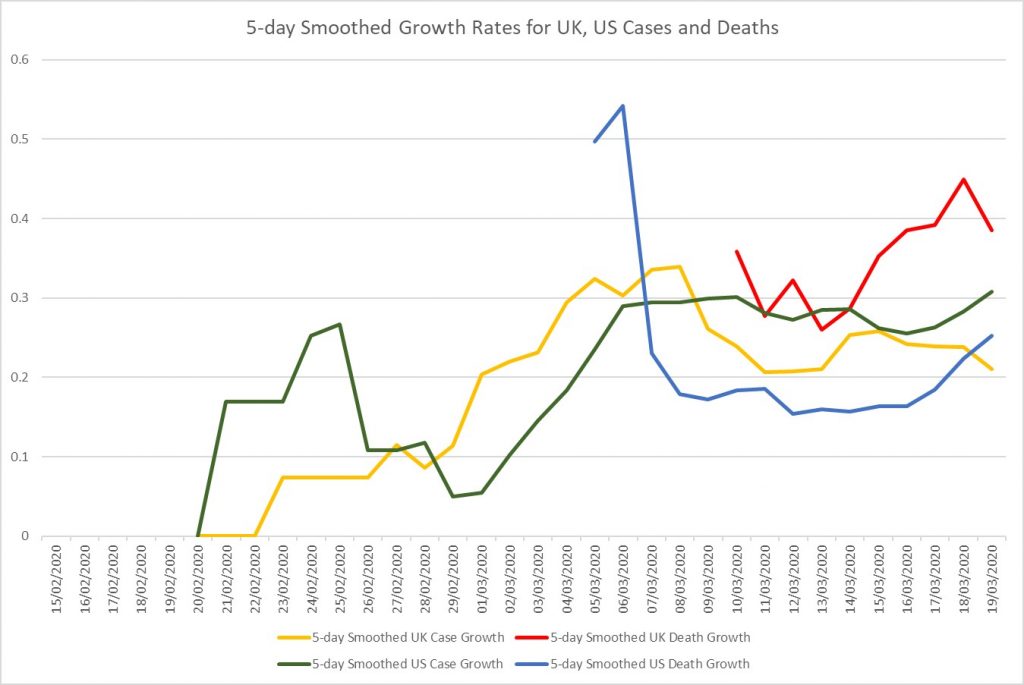
The chart below (Chart 2) tracks the growth rates of UK and US cases and deaths over time. To reduce the fluctuations in the lines I have plotted for each day an average of the previous 5 days’ growth rates. This demonstrates very clearly the higher than expected growth rate of deaths in the UK, although it shows too that the growth rate of US deaths is also increasing. If efforts to tackle infection spread and protect those particularly vulnerable are being effective we would hope to see a downward shift in these growth rates, particularly those in the number of deaths, very soon.
Suppression Policy in the UK
Estimates from the Imperial College team suggest that infection fatality increases markedly with age. The risk of death from Covid-19 is estimated at 0.03% for those aged 20-29, 0.6% for those aged 50-59, 5% for those aged 70-79 and over 9% for those 80 years and older. Their proposed strategies reflect this age-related vulnerability. They consider the following:
- Case isolation in the home – Symptomatic cases to stay at home for 7 days.
- Voluntary home quarantine – Following identification of a symptomatic case in the household, all household members remain at home for 14 days.
- Social distancing of those over 70 years of age – Reduce contacts by 50% in workplaces, increase household contacts by 25% and reduce other contacts by 75%.
- Social distancing of entire population – All households reduce contact outside household, school or workplace by 75%. School contact rates are unchanged and workplace contact rates reduced by 25%.
- Closure of schools and universities – Closure of all schools and 25% of universities to remain open.
As a baseline, their modelling of the Coronavirus epidemic from estimates of the observed pattern of infection so far is that without any intervention there would be a peak in mortality (daily deaths) after approximately 3 months, by which time around 80% of the UK (and US) populations would have been infected. Without taking into account the inevitable overwhelming of healthcare systems (with ICU demand over 30 times greater than the maximum supply), around 500,000 deaths in the UK and over 2 million in the US are predicted.
An ‘Adaptive’ Policy
In the team’s modelling they come to the conclusion that to avoid overwhelming numbers of cases a ‘combination of case isolation, social distancing of the entire population and either household quarantine or school and university closure are required’ with school and university closure being more effective. Because these policies may need to be maintained for many months (essentially until an effective vaccine becomes widely available) they propose an ‘adaptive’ policy in which social distancing and school and university closure are only initiated after weekly confirmed case incidence in ICU patients exceeds a particular threshold, or ‘trigger’. These measures would then be relaxed when ICU cases fall again below a certain level. The lower the trigger the fewer the deaths, but they estimate 200 ICU cases per week may be the lowest trigger point that keeps peak ICU demand below ‘surge limits’. In this case, these measures would be in place for perhaps two-thirds of the time before a vaccine is available.
The Imperial College team estimate a typical delay of 2-3 weeks between the introduction of interventions and an observable impact on hospitalised case numbers, which means early action before COVID-19 admissions reach the trigger 200 per week.
They end their report with the following caveat.
However, we emphasise that is not at all certain (sic) that suppression will succeed long term; no public health intervention with such disruptive effects on society has been previously attempted for such a long duration of time. How populations and societies will respond remains unclear.